
Our Daughters Foundation
FAQs: Get Your Endometriosis Questions Answered
From diagnosis delays to treatment options, find straightforward answers to the questions you have about endometriosis.
FAQs: Get Your Endometriosis Questions Answered
From diagnosis delays to treatment options, find straightforward answers to the questions you have about endometriosis.
What is endometriosis, and is it considered a menstrual disease?
Endometriosis is a systemic, inflammatory condition characterized by tissue similar to the lining of the uterus growing in other parts of the body. Endometriosis has been found in every organ. It is not simply a menstrual disease, yet is often mischaracterized as such, even by reputable sources.
Approximately how many people are affected by endometriosis, and what are some common symptoms they may experience?
Endometriosis affects approximately 1 in 10 women. Common symptoms include, but are not limited to, pelvic pain any time during the month, a wide range of GI symptoms, urinary symptoms, fatigue, debilitating periods and more depending on where the endometriosis lesions are located in the body.
What is the average diagnostic delay for endometriosis, and what factors contribute to this delay?
Symptoms often start early in life, but due to cultural taboos, misinformation and a historical lack of emphasis in medical education, they may be ignored or misdiagnosed by caregivers, healthcare consumers and practitioners alike. The average diagnostic delay is 7-10 years.
When can endometriosis symptoms begin, and what percentage of teenagers withchronic pelvic pain may have the condition?
Endometriosis symptoms may begin as early as when puberty starts. Endometriosis symptoms can present before menstruation, during menstruation, and/or after menstruation. An estimated 70% of teens with chronic pelvic pain go on to be later diagnosed with endometriosis.
What constitutes a "red flag" regarding pelvic pain, and what action should be taken if someone experiences this?
Red flag: If you or your patient regularly feels pain during or around periods, and this pain is bad enough to interfere with usual activities, this is a red flag - it is not normal and should be investigated further as soon as possible. (If you do not have this, it doesn't mean that you don't have endometriosis).
Identified risk factors for developing endometriosis.
Risk factors for endometriosis include a mother or sister having the disease (7x increased risk), early onset of menses, short or frequent menstrual cycles, Mullerian abnormalities, autoimmune conditions and more. However, many people develop endo who have none of these risk factors.
Is a hysterectomy considered a cure for endometriosis, and is pregnancy a cure?
Hysterectomy is not a cure for endometriosis. A disease characterized by tissue found outside of the uterus is not cured by removal of the uterus, ovaries and/or tubes and cervix. Over 100,000 hysterectomies are performed each year in the United States for endometriosis and most of them are unnecessary. Neither is pregnancy a cure for endometriosis.
Why are individualized, multi-disciplinary treatment plans needed for endometriosis, and which specialist should be consulted?
People with endometriosis need an individualized, multi-disciplinary treatment plan that may include specialized, incredibly difficult surgery. Most gynecologists are not trained in advanced endometriosis cases. Drug therapy may suppress symptoms, yet it does not eradicate endometriosis. Patients should be referred to an endometriosis specialist. We cannot emphasize this enough, please go to a an endometriosis specialist. Your regular OB/GYN should refer you to one if they suspect you have endo.
What are some common co-morbidities associated with endometriosis?
People with endometriosis have an increased risk of co-morbidities including allergies, asthma, and chemical sensitivities, autoimmune diseases such as multiple sclerosis and lupus, chronic fatigue syndrome and fibromyalgia, and certain cancers, such as ovarian and breast cancer. Many doctors are also seeing MCAS, POTS and hEDS as common co-morbidities.
How does endometriosis impact quality of life beyond physical symptoms, and what holistic approach is recommended?
Endometriosis often reduces quality of life and contributes to psychological distress. Unnecessary delays in diagnosis and gaslighting contribute to the negative mental health impacts of the disease. A holistic approach to care including mental health support can improve quality of life.
What is endometriosis, and is it considered a menstrual disease?
Endometriosis is a systemic, inflammatory condition characterized by tissue similar to the lining of the uterus growing in other parts of the body. Endometriosis has been found in every organ. It is not simply a menstrual disease, yet is often mischaracterized as such, even by reputable sources.
Approximately how many people are affected by endometriosis, and what are some common symptoms they may experience?
Endometriosis affects approximately 1 in 10 people born with female reproductive organs. Common symptoms include, but are not limited to, pelvic pain any time during the month, a wide range of GI symptoms, urinary symptoms, fatigue, debilitating periods and more depending on where the endometriosis lesions are located in the body.
What is the average diagnostic delay for endometriosis, and what factors contribute to this delay?
Symptoms often start early in life, but due to cultural taboos, misinformation and a historical lack of emphasis in medical education, they may be ignored or misdiagnosed by caregivers, healthcare consumers and practitioners alike. The average diagnostic delay is 7-10 years.
When can endometriosis symptoms begin, and what percentage of teenagers withchronic pelvic pain may have the condition?
Endometriosis symptoms may begin as early as when puberty starts. Endometriosis symptoms can present before menstruation, during menstruation, and/or after menstruation. An estimated 70% of teens with chronic pelvic pain go on to be later diagnosed with endometriosis.
What constitutes a "red flag" regarding pelvic pain, and what action should be taken if someone experiences this?
Red flag: If you or your patient regularly feels pain during or around periods, and this pain is bad enough to interfere with usual activities, this is a red flag - it is not normal and should be investigated further as soon as possible. (If you do not have this, it doesn't mean that you don't have endometriosis).
Identified risk factors for developing endometriosis.
Risk factors for endometriosis include a mother or sister having the disease (7x increased risk), early onset of menses, short or frequent menstrual cycles, Mullerian abnormalities, autoimmune conditions and more. However, many people develop endo who have none of these risk factors.
Is a hysterectomy considered a cure for endometriosis, and is pregnancy a cure?
Hysterectomy is not a cure for endometriosis. A disease characterized by tissue found outside of the uterus is not cured by removal of the uterus, ovaries and/or tubes and cervix. Over 100,000 hysterectomies are performed each year in the United States for endometriosis and most of them are unnecessary. Neither is pregnancy a cure for endometriosis.
Why are individualized, multi-disciplinary treatment plans needed for endometriosis, and which specialist should be consulted?
People with endometriosis need an individualized, multi-disciplinary treatment plan that may include specialized, incredibly difficult surgery. Most gynecologists are not trained in advanced endometriosis cases. Drug therapy may suppress symptoms, yet it does not eradicate endometriosis. Patients should be referred to an endometriosis specialist.
What are some common co-morbidities associated with endometriosis?
People with endometriosis have an increased risk of co-morbidities including allergies, asthma, and chemical sensitivities, autoimmune diseases such as multiple sclerosis and lupus, chronic fatigue syndrome and fibromyalgia, and certain cancers, such as ovarian and breast cancer.
How does endometriosis impact quality of life beyond physical symptoms, and what holistic approach is recommended?
Endometriosis often reduces quality of life and contributes to psychological distress. Unnecessary delays in diagnosis and gaslighting contribute to the negative mental health impacts of the disease. A holistic approach to care including mental health support can improve quality of life.
What the Largest Genetic Study of Endo Actually Means
Why This Study Caught My Attention
One of the questions I hear most often is, "If researchers have known for years that endometriosis has a genetic component, why don't we have better answers?"
For many years, researchers have recognized that endometriosis tends to run in families. Women with a close relative who has endometriosis are at a higher risk of developing the disease themselves. Studies of twins have also suggested that genetics plays an important role. But knowing that a disease has a genetic component is very different from understanding which genes are involved or how those genes influence the disease. That's why this new study is so important.
Researchers analyzed genetic data from more than1.4 million women, including105,869 women with endometriosis. This makes it the largest genetic study of endometriosis ever conducted.
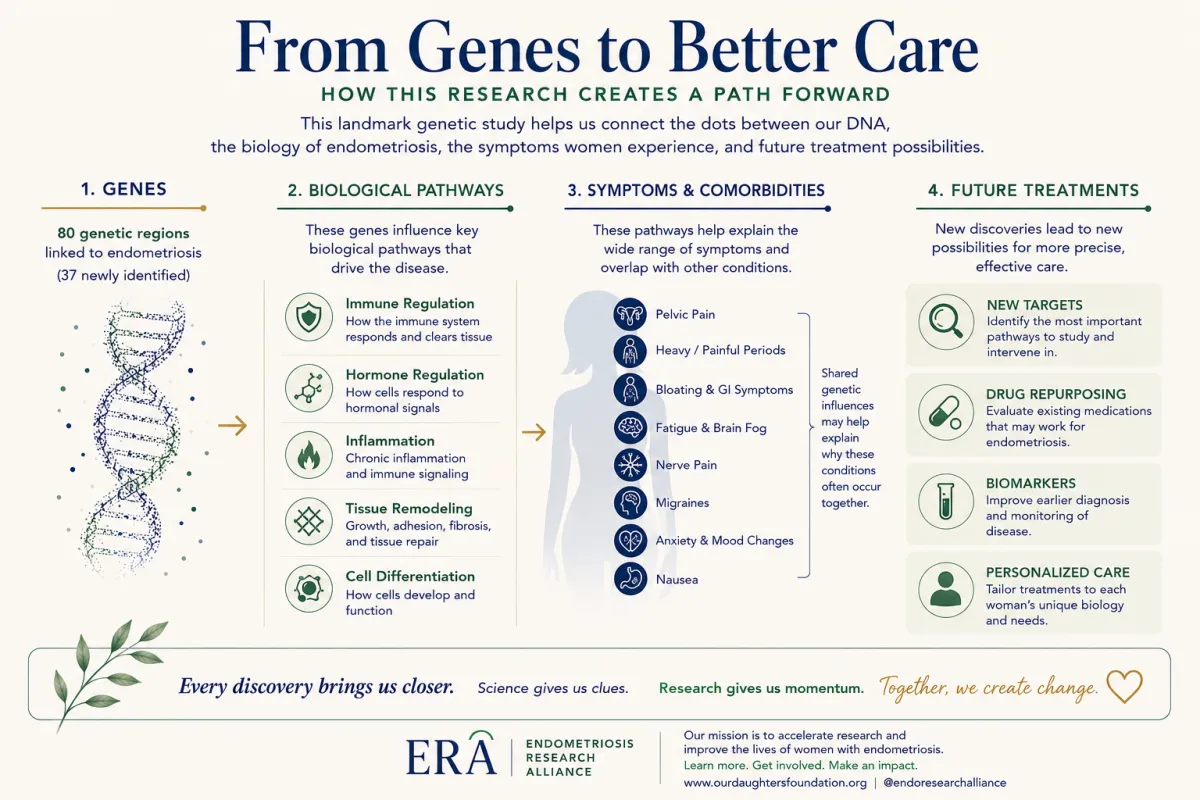
This study didn't reveal a single "endometriosis gene." In fact, that wasn't what researchers expected to find. Instead, they identified 80 regions of the genome associated with endometriosis, including37 regions that had not previously been linked to the disease. Each of these regions offers another clue about the biology of endometriosis and another place for researchers to investigate.
Rather than confirming that endometriosis is caused by one abnormal gene or one malfunctioning process, it reinforces what many clinicians and researchers have been observing for years: endometriosis is a complex disease involving many biological systems working together.
No two women experience endo in the say way. Some struggle primarily with pelvic pain. Others battle infertility. Some develop bowel, bladder, or nerve involvement. Many live with fatigue, migraine, or other conditions that seem connected but have been difficult to explain. This study doesn't answer all of those questions, but it begins to show why those differences may exist.
Why Do Genes Matter If Genes Aren't Treatments?
This may be one of the most important questions to ask. Finding a genetic region associated with endometriosis does not mean researchers have discovered a treatment, nor does it necessarily mean they have identified the specific gene responsible. Instead, it provides an important clue about where to look next.
Imagine someone tells you that you're looking for a particular house somewhere in the United States. That would be an overwhelming search. Now imagine they narrow the location to a single city, then to a neighborhood, and eventually to a specific street. With each new piece of information, the search becomes more focused. That is essentially what studies like this accomplish. They don't identify the final answer, but they help researchers narrow their search and concentrate on the areas most likely to provide meaningful insights.
Once researchers know where to look, they can begin asking more targeted questions. What proteins are produced in this region? How might these genes influence inflammation or immune function? Do they affect the way cells respond to hormones? Could one of these biological pathways already be influenced by a medication that has been developed for another condition? These are the types of questions that move research forward.
Scientific progress rarely comes from a single discovery. More often, each study provides new information that allows researchers to ask better questions, design more focused experiments, and build upon what has already been learned. In that respect, this study provides an important foundation for the research that comes next.
One of the privileges of serving through Our Daughters Foundation has been getting to know many of the researchers who have dedicated their careers to women's health. In fact we are supporting a research project on genetics currently at Cold Springs Harbor Lab (The Our Daughters Foundation Genomics Initiative with Dr. Semir Bayez) Reading studies like this has also given me a greater appreciation for how scientific progress actually happens.
Research is rarely a straight path from discovery to treatment. More often, each study answers one question while raising several others. Researchers build on previous work, test new ideas, compare results, and continually refine their understanding as new evidence emerges. That process can feel slow, particularly for women who are living with chronic pain and hoping for better answers, but it is also what gives us confidence in the discoveries that eventually shape patient care.
This study is a good example of that process. It doesn't provide all the answers, nor do the authors suggest that it does. What it offers is a clearer understanding of the biological pathways involved in endometriosis and a stronger foundation for future research. Identifying new genetic regions, exploring how those regions influence disease, and investigating whether existing medications may affect those pathways are all important steps toward developing more precise diagnostic tools and treatment options.
That is one of the reasons Our Daughters Foundation continues to invest in research. Every carefully designed study expands our understanding of this disease and helps move the field forward. While progress may not always happen as quickly as we would like, today's discoveries often become the foundation for tomorrow's advances.
What Did Researchers Learn?
One of the strengths of this study is that it didn't stop with identifying genetic regions. The researchers also looked at what those genetic regions actually do.
Many of the newly identified regions are involved in biological pathways that have long been suspected to play a role in endometriosis. Rather than pointing to one single cause, the findings reinforce the idea that endometriosis develops through the interaction of several different systems within the body.
Let's look at those pathways one at a time.
The Immune System
Our immune system does far more than fight infections. It also helps regulate inflammation, removes damaged cells, and responds to tissue injury.
This study identified several genetic regions involved in immune regulation. While researchers are still working to understand exactly how these genes influence endometriosis, the findings support the growing body of evidence that the immune system is actively involved in the disease.
For many years, researchers have asked why endometriosis lesions are able to implant, grow, and persist in some women. One possibility is that differences in immune signaling contribute to the body's response to those lesions. This study doesn't answer that question completely, but it gives researchers additional pathways to investigate.
Hormone Signaling
Most women with endometriosis know that hormones play a role in the disease. Estrogen, in particular, has been studied extensively.
What's becoming increasingly clear, however, is that hormone biology is much more complicated than simply having "too much estrogen."
Cells throughout the body contain receptors that determine how they respond to hormones. The genetic differences identified in this study may influence those responses. That could help explain why hormonal treatments are very effective for some women, less effective for others, and not tolerated by some at all.
Researchers are continuing to study these differences as they work toward more individualized treatment approaches.
Inflammation
Inflammation is one of the most consistently observed features of endometriosis.
When inflammation becomes chronic, it can affect far more than the tissue where it begins. It influences pain signaling, healing, immune function, and communication between cells.
This study identified genetic pathways involved in inflammatory signaling, adding further evidence that inflammation is not simply a consequence of endometriosis. It appears to be an important part of the disease process itself.
Understanding those pathways may eventually help researchers identify new ways to reduce inflammation more precisely than is possible today.
Tissue Remodeling and Fibrosis
This section particularly caught my attention because it reflects what many expert excision surgeons see every day in the operating room.
Endometriosis isn't always made up of superficial lesions. In many women, the disease is associated with fibrosis, scarring, adhesions, and changes to surrounding tissue.
Researchers identified genes involved in tissue remodeling, which is the process by which tissue repairs, reorganizes, and sometimes scars after injury or inflammation.
Learning more about these pathways may help explain why some women develop extensive fibrosis while others do not. It may also provide future opportunities to better understand deep infiltrating disease and the long-term effects of chronic inflammation.
Cell Differentiation
Every cell in our body receives instructions that influence how it grows, develops, and functions.
Researchers also found genetic regions involved in cell differentiation, the process that helps determine how cells mature and respond to their environment.
Although this area is still being explored, it may help explain why endometriosis can behave differently from one patient to another and why lesions themselves can vary in appearance and activity.
A Disease Influenced by Many Systems
As I read through these findings, one thought kept coming back to me.
For years, women have described symptoms that extend well beyond painful periods. They have talked about fatigue, bowel symptoms, bladder symptoms, nerve pain, inflammation, and a wide variety of experiences that don't always fit into a simple description of endometriosis.
This study doesn't prove that all of those symptoms come from the same biological process. It does, however, reinforce the idea that endometriosis is a complex disease involving many interconnected systems.
To me, that's an important distinction.
The science isn't making the disease more complicated than patients have experienced it.
It's helping explain why many women have experienced it as a complex disease all along.
What About Adenomyosis?
Another finding that deserves attention is the discovery offive genetic regions shared between endometriosis and adenomyosis.
Many women are diagnosed with both conditions, yet historically they have often been studied separately.
Finding shared genetic regions doesn't mean the diseases are identical. They are distinct conditions with important differences.
What it does suggest is that they may share some of the same underlying biological mechanisms.
That opens the door to new questions.
Could studying one disease help us better understand the other?
Could future therapies target pathways involved in both conditions?
Those answers aren't available yet, but studies like this help researchers know where to look next.
Looking Beyond Endometriosis
One section of the paper I found particularly interesting examined conditions that commonly occur alongside endometriosis.
Researchers identified shared genetic associations with symptoms and conditions including abdominal pain, migraine, anxiety, and nausea.
For women living with endometriosis, it also reinforces something many have experienced personally: our health doesn't always fit neatly into separate boxes. The body functions as an integrated system, and research is increasingly reflecting that reality.
One of the Most Encouraging Areas: Drug Repurposing
If there was one part of this study that made me stop and think, it was the discussion of drug repurposing.
Developing a brand-new medication is an incredibly long process. It often takes many years of research before a drug reaches patients. Drug repurposing asks a different question.
Instead of starting from the beginning, researchers ask whether medications that already exist might influence the biological pathways involved in endometriosis. Using the genetic information from this study, researchers identified several classes of existing medications that deserve further investigation, including drugs currently used in breast cancer treatment, contraception, and prevention of preterm birth.
If future studies demonstrate that one of these medications safely benefits women with endometriosis, the path to clinical use could potentially be shorter than developing an entirely new drug from the beginning.
That's why so many researchers are interested in drug repurposing. It offers another pathway toward better treatments while building on medications that are already well understood.
Why This Study Matters
As I finished reading this paper, I found myself thinking less about the individual genetic regions and more about the direction of the research itself.
Over the past decade, our understanding of endometriosis has changed significantly. Researchers are moving beyond asking whether genetics plays a role in the disease and are now identifying specific biological pathways that deserve further investigation. Studies like this help explain why endometriosis can present so differently from one woman to another and provide new opportunities to investigate targeted therapies, improved diagnostics, and potential drug repurposing.
I also appreciate the restraint of the authors. They are careful to distinguish between what their data demonstrate and what still requires additional study. In an era when scientific findings are often overstated in headlines, that careful approach is worth recognizing. This paper identifies promising directions for future research without suggesting that questions have been answered before the evidence is available.
For those of us who follow endometriosis research closely, that may be one of the most encouraging aspects of the study. It reflects a field that continues to mature, asks increasingly sophisticated questions, and is building upon decades of previous work.
A Few Thoughts That Stayed With Me
Rather than trying to summarize the entire paper in a few sentences, these are the ideas I found myself returning to after reading it.
The first is that endometriosis continues to reveal itself as a biologically complex disease. The interaction between genetics, immune regulation, hormone signaling, inflammation, fibrosis, and tissue remodeling reinforces the importance of studying these systems together rather than in isolation.
The second is that collaboration across disciplines is becoming increasingly important. Geneticists, immunologists, surgeons, reproductive endocrinologists, pain researchers, and basic scientists are each contributing pieces of the same puzzle. Studies like this remind us that meaningful progress often comes from connecting discoveries across multiple fields of research.
The third is that identifying biological pathways creates opportunities to ask better research questions. Some of those questions may eventually lead to new diagnostics. Others may lead to therapies that target specific mechanisms involved in the disease. Some may not. That is the nature of scientific discovery, and it is one of the reasons replication and continued investigation are so important.
Finally, this paper reinforces why research deserves continued investment. Every well-designed study adds to a growing body of knowledge that researchers around the world are building together. While no single paper changes clinical practice overnight, each contributes to a stronger scientific foundation for the work that follows.
Primary Research
Koller D, He J, Løkhammer S, et al.Multi-ancestry genome-wide association and integrated multi-omics analyses of endometriosis and its clinical manifestations.Nature Genetics.2026.
Additional Reading
Yale School of Medicine.Largest-Ever Genetic Study of Endometriosis Uncovers 80 Risk Regions and New Avenues for Treatment.
Rahmioglu N, et al.The genetic basis of endometriosis and comorbidity with other pain and inflammatory conditions.Nature Genetics.2023.
Krina T. Zondervan, Christian M. Becker, and Stacey A. Missmer.Endometriosis.Nature Reviews Disease Primers. 2018.
Consensus publications from the World Endometriosis Society on research priorities and future directions.

Join Us: Make a Difference Today
Your support can transform lives. Every donation helps us fund research, advocate for better care, and provide essential grants to women facing debilitating conditions.
Join Us: Make a Difference Today
Your support can transform lives. Every donation helps us fund research, advocate for better care, and provide essential grants to women facing debilitating conditions.