
The Overlooked Link: Allen-Masters Syndrome and Endometriosis
How a Little-Known Condition Can Complicate Diagnosis and Treatment for Women in Pain
The Overlooked Link: Allen-Masters Syndrome and Endometriosis
How a Little-Known Condition Can Complicate Diagnosis and Treatment for Women in Pain
What Is Allen-Masters Syndrome?
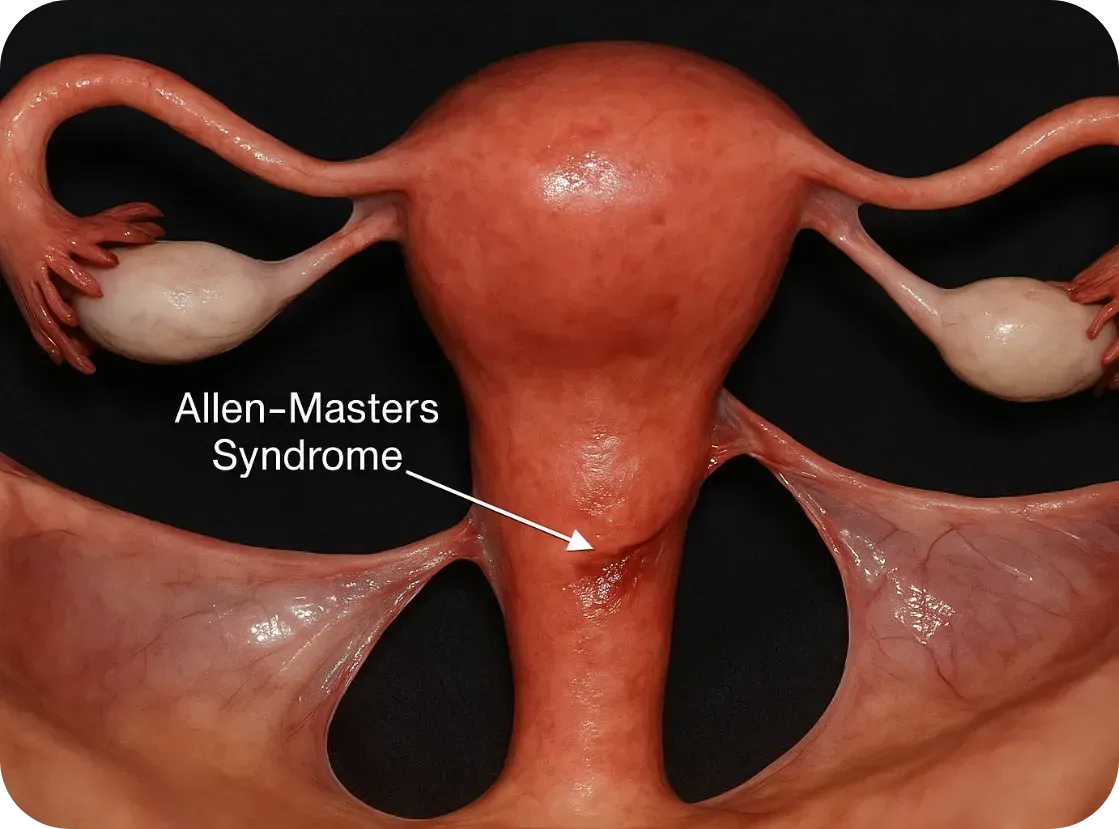
Allen-Masters Syndrome (AMS) refers to a condition where the ligaments that support the uterus become torn or stretched, often due to trauma or childbirth. The damage causes the uterus to become hypermobile, or “floppy,” which can lead to chronic pelvic pain, abnormal uterine positioning, and a range of gynecological symptoms.
First described in the 1950s by gynecologists Allen and Masters, the syndrome was initially observed in women who experienced difficult or forceful deliveries. However, it's now known that other pelvic trauma—such as surgeries, repeated inflammation, or even invasive endometriosis—can also play a role.
How It Feels: The Symptoms
The symptoms of AMS often overlap with other pelvic disorders, including endometriosis, which makes it incredibly hard to diagnose:
• Chronic pelvic pain, especially on one side
• Pain during intercourse (dyspareunia)
• A feeling of “heaviness” or dragging in the pelvis
• Irregular bleeding or spotting
• Referred pain to the lower back or legs
• Pain made worse by certain movements or positions
These symptoms can persist even after surgery for endometriosis or fibroids, leaving women frustrated and wondering why their treatments didn’t work.
The Complication with Endometriosis
Endometriosis and Allen-Masters Syndrome can coexist—and when they do, they complicate each other.

Endometriosis and Allen-Masters Syndrome can coexist—and when they do, they complicate each other.
Here’s how:
1. Mimicking or Masking Each Other
AMS pain can feel nearly identical to endometriosis. In laparoscopic surgery, torn ligaments or peritoneal defects might be mistaken for endometriosis—or missed entirely.
2. Worsening Each Other
The uterine instability caused by AMS may increase friction and inflammation in the pelvis, potentially exacerbating endometriosis symptoms. Likewise, the invasive nature of endometriosis can weaken uterine ligaments, creating a cycle of worsening pain.
3. Delaying Diagnosis
Because AMS isn’t well known, many surgeons focus only on excising visible endometriosis lesions. If ligament tears or pelvic instability aren’t also addressed, pain may persist despite "successful" surgery.
4. Influencing Fertility
While endometriosis is a known contributor to infertility, AMS can add to the challenge by altering the position of the uterus, interfering with sperm transport, or making embryo implantation more difficult.
Diagnosis: Why It’s Often Missed
AMS is best diagnosed through clinical examination and often requires a high index of suspicion from an experienced gynecologic surgeon. Imaging like MRI or ultrasound may not show ligament damage clearly. In some cases, laparoscopic exploration is the only way to confirm it, by observing a hypermobile uterus or peritoneal defects (like dimples or windows in the pelvic lining).
Unfortunately, many OB/GYNs are not trained to look for Allen-Masters Syndrome, which means it’s often overlooked—especially in patients already diagnosed with endometriosis
What Can Be Done?
If AMS is suspected, the treatment may include:
• Pelvic physical therapy to support surrounding muscles and reduce pain
• Surgical repair or suspension of the damaged ligaments, often during laparoscopy
• Pain management strategies including nerve blocks or hormonal regulation if endometriosis is also present
• Lifestyle modifications to reduce strain on the pelvis (avoiding certain exercises, managing constipation, etc.)

The Takeaway
Allen-Masters Syndrome may not be as well-known as endometriosis, but its impact is very real—especially for women who feel like they've tried everything and still have no answers.
If you’ve had surgery for endometriosis and your pain persists, or if your symptoms don’t quite fit the typical endo profile, it might be worth asking your doctor about Allen-Masters Syndrome.
Women deserve full answers—not partial relief.
Sources & Further Reading
• Howard FM. (2003). Chronic Pelvic Pain. Obstetrics and Gynecology
• Vercellini P et al. (2006). Chronic pelvic pain: pathogenesis and therapy. Best Practice & Research Clinical Obstetrics and Gynaecology
• Tu FF et al. (2017). Beyond Endometriosis: Recognizing and Treating Comorbid Pelvic Pain Disorders. Clinical Obstetrics and Gynecology
What Is Allen-Masters Syndrome?
Allen-Masters Syndrome (AMS) refers to a condition where the ligaments that support the uterus become torn or stretched, often due to trauma or childbirth. The damage causes the uterus to become hypermobile, or “floppy,” which can lead to chronic pelvic pain, abnormal uterine positioning, and a range of gynecological symptoms.
First described in the 1950s by gynecologists Allen and Masters, the syndrome was initially observed in women who experienced difficult or forceful deliveries. However, it's now known that other pelvic trauma—such as surgeries, repeated inflammation, or even invasive endometriosis—can also play a role.
How It Feels: The Symptoms
The symptoms of AMS often overlap with other pelvic disorders, including endometriosis, which makes it incredibly hard to diagnose:
• Chronic pelvic pain, especially on one side
• Pain during intercourse (dyspareunia)
• A feeling of “heaviness” or dragging in the pelvis
• Irregular bleeding or spotting
• Referred pain to the lower back or legs
• Pain made worse by certain movements or positions
These symptoms can persist even after surgery for endometriosis or fibroids, leaving women frustrated and wondering why their treatments didn’t work.
The Complication with Endometriosis
Endometriosis and Allen-Masters Syndrome can coexist—and when they do, they complicate each other.
Endometriosis and Allen-Masters Syndrome can coexist—and when they do, they complicate each other.
Here’s how:
1. Mimicking or Masking Each Other
AMS pain can feel nearly identical to endometriosis. In laparoscopic surgery, torn ligaments or peritoneal defects might be mistaken for endometriosis—or missed entirely.
2. Worsening Each Other
The uterine instability caused by AMS may increase friction and inflammation in the pelvis, potentially exacerbating endometriosis symptoms. Likewise, the invasive nature of endometriosis can weaken uterine ligaments, creating a cycle of worsening pain.
3. Delaying Diagnosis
Because AMS isn’t well known, many surgeons focus only on excising visible endometriosis lesions. If ligament tears or pelvic instability aren’t also addressed, pain may persist despite "successful" surgery.
4. Influencing Fertility
While endometriosis is a known contributor to infertility, AMS can add to the challenge by altering the position of the uterus, interfering with sperm transport, or making embryo implantation more difficult.
Diagnosis: Why It’s Often Missed
AMS is best diagnosed through clinical examination and often requires a high index of suspicion from an experienced gynecologic surgeon. Imaging like MRI or ultrasound may not show ligament damage clearly. In some cases, laparoscopic exploration is the only way to confirm it, by observing a hypermobile uterus or peritoneal defects (like dimples or windows in the pelvic lining).
Unfortunately, many OB/GYNs are not trained to look for Allen-Masters Syndrome, which means it’s often overlooked—especially in patients already diagnosed with endometriosis
What Can Be Done?
If AMS is suspected, the treatment may include:
• Pelvic physical therapy to support surrounding muscles and reduce pain
• Surgical repair or suspension of the damaged ligaments, often during laparoscopy
• Pain management strategies including nerve blocks or hormonal regulation if endometriosis is also present
• Lifestyle modifications to reduce strain on the pelvis (avoiding certain exercises, managing constipation, etc.)
The Takeaway
Allen-Masters Syndrome may not be as well-known as endometriosis, but its impact is very real—especially for women who feel like they've tried everything and still have no answers.
If you’ve had surgery for endometriosis and your pain persists, or if your symptoms don’t quite fit the typical endo profile, it might be worth asking your doctor about Allen-Masters Syndrome.
Women deserve full answers—not partial relief.
Sources & Further Reading
• Howard FM. (2003). Chronic Pelvic Pain. Obstetrics and Gynecology
• Vercellini P et al. (2006). Chronic pelvic pain: pathogenesis and therapy. Best Practice & Research Clinical Obstetrics and Gynaecology
• Tu FF et al. (2017). Beyond Endometriosis: Recognizing and Treating Comorbid Pelvic Pain Disorders. Clinical Obstetrics and Gynecology
Join Us: Make a Difference Today
Your support can transform lives. Every donation helps us fund research, advocate for better care, and provide essential grants to women facing debilitating conditions.
Join Us: Make a Difference Today
Your support can transform lives. Every donation helps us fund research, advocate for better care, and provide essential grants to women facing debilitating conditions.
Relaxing Your Pelvic Floor
Relaxing the Pelvic Floor: Simple Practices with Powerful Benefits
Tension in the pelvic floor is more common than many realize—and it can be a significant source of pain, dysfunction, and stress. While most people have heard of Kegels to strengthen pelvic floor muscles, the equally important skill of relaxing those muscles is often overlooked. Chronic tightness in the pelvic floor can lead to a range of symptoms including pelvic pain, urinary urgency, painful intercourse, constipation, and low back pain.
*Your pelvic floor carries a lot—physically and emotionally. Incorporating simple tools like these into your daily routine isn’t just about relief after symptoms hit—it’s about building a system that might help prevent them before they start. A few minutes of deep breathing, gentle movement, or a warm bath can help calm your nervous system, ease tension, and support your body.That said, flare-ups aren’t always in your control—and that doesn’t mean you’re doing anything wrong. This is the nature of endometriosis. These are just supportive tools, not a cure—but sometimes, little things can make a big difference.
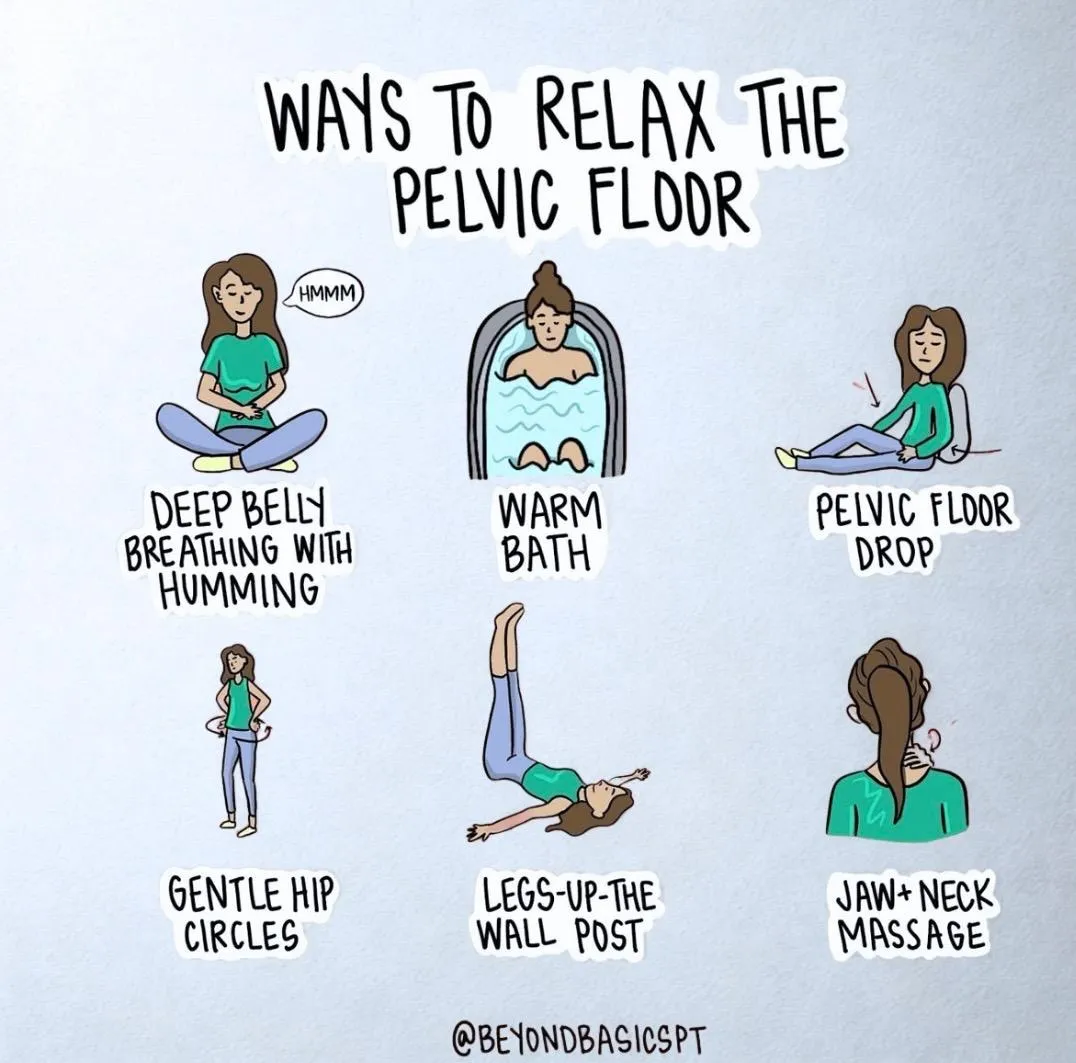
Fortunately, simple daily techniques—like the ones illustrated by @beyondbasicspt in the graphic above—can make a profound difference. Let’s break down each method and explore what the research says.
1. Deep Belly Breathing with Humming
Slow diaphragmatic breathing encourages the pelvic floor to relax naturally. When you inhale deeply, your diaphragm moves downward, and this movement is mirrored by the pelvic floor, creating a gentle stretch and release.
Why add humming? Humming stimulates the vagus nerve, which activates the parasympathetic nervous system (the “rest and digest” response), helping the entire pelvic region soften.
Research Insight: A 2020 study published in Pain Medicine found that slow, diaphragmatic breathing improved outcomes in patients with chronic pelvic pain by reducing muscle tone and improving nervous system regulation (Mehling et al., 2020).
2. Warm Bath
Immersion in warm water increases blood flow and reduces muscle guarding—especially in the pelvic area. The buoyancy also helps reduce gravitational compression, encouraging muscle relaxation.
Research Insight: Hydrotherapy has long been shown to reduce muscle tension and improve circulation (Kamioka et al., 2010). For pelvic pain specifically, warmth and hydrostatic pressure may help ease myofascial tension in the pelvic floor.
3. Pelvic Floor Drop (Let-Go Technique)
Unlike Kegels (which focus on contraction), the pelvic floor drop emphasizes releasing and lengthening the pelvic muscles. Think of it as the "exhale and let go" moment for the pelvic floor.
Research Insight: A 2016 review in the Journal of Bodywork and Movement Therapies emphasizes that relaxation techniques—including conscious "letting go"—are key in treating non-relaxing pelvic floor dysfunction (FitzGerald et al., 2016).
4. Gentle Hip Circles
These rhythmic movements help mobilize the hips and pelvis, gently loosening fascia and improving circulation in the pelvic region.
Research Insight: Movement therapies that increase pelvic mobility are beneficial in reducing hypertonicity (muscle overactivity) in the pelvic floor (Haugstad et al., 2006).
5. Legs-Up-The-Wall Pose
Known as Viparita Karani in yoga, this pose promotes venous return and encourages full-body relaxation. It also reduces pressure in the pelvic region and helps calm the nervous system.
Research Insight: A 2013 study in Evidence-Based Complementary and Alternative Medicine noted that restorative yoga poses, like legs-up-the-wall, reduce sympathetic nervous system activity and improve muscle tone regulation (Telles et al., 2013).
6. Jaw + Neck Massage
Here’s a fascinating link: the jaw and the pelvic floor are neurologically and developmentally connected. Tension in one area often reflects or reinforces tension in the other.
Tip: Try gently massaging the base of your skull and jawline—or even releasing your tongue from the roof of your mouth—to help the pelvic muscles relax.
Research Insight: Somatic connections between the jaw and pelvis have been observed in body-oriented therapies. A 2021 review published in Medical Hypotheses proposed shared motor control pathways that link craniofacial and pelvic floor muscle groups (Wallden, 2021).
Final Thoughts
Pelvic floor relaxation isn’t just about relieving pain—it’s about restoring balance, function, and a sense of ease in the body. Whether you’re dealing with pelvic pain, recovering from childbirth, or simply seeking more mind-body awareness, these gentle practices are worth integrating into your daily routine.
As always, if you're experiencing persistent pelvic discomfort, consult a pelvic floor physical therapist for a personalized plan. These professionals can guide you through both strengthening and relaxation techniques safely.
References
Mehling, W. E., et al. (2020). Effects of breathing retraining on chronic pelvic pain. Pain Medicine, 21(4), 798–808.
Kamioka, H., et al. (2010). Effectiveness of aquatic exercise and balneotherapy: A summary of systematic reviews. Journal of Epidemiology, 20(1), 2–12.
FitzGerald, M. P., et al. (2016). Evaluation and treatment of non-relaxing pelvic floor dysfunction. J Bodyw Mov Ther, 20(2), 275–281.
Haugstad, G. K., et al. (2006). Muscular and non-muscular responses to movement therapy in women with chronic pelvic pain. Physiotherapy Research International, 11(4), 217–228.
Telles, S., et al. (2013). Restorative yoga for women with pelvic pain: a randomized controlled trial. Evid Based Complement Alternat Med, 2013, 792581.
Wallden, M. (2021). The anatomical and neurobiological link between the jaw and pelvic floor. Medical Hypotheses, 150, 110556.
